Stage III papillary thyroid cancer
Stage III is papillary carcinoma in patients older than 45 years that is larger than 4 cm and is limited to the thyroid or with minimal extrathyroid extension, or positive lymph nodes limited to the pretracheal, paratracheal, or prelaryngeal/Delphian nodes. Papillary carcinoma that has invaded adjacent cervical tissue has a worse prognosis than tumors confined to the thyroid.
----------------Pathology report
tumor #1 with focal extension into soft tissue immediately surrounding thyroid.
发表者:龙斌 3179人已访问
any staging methods have been developed in order to predict the prognosis for a patient with differentiated thyroid cancer. These methods quantify various characteristics of the individual tumor as well as the patient. Fortunately most types of thyroid cancer have an excellent prognosis. Unlike other types of cancer, the prognosis of differentiated thyroid cancer largely depends on the age of the patient at the time it is diagnosed. Thyroid cancers which are not differentiated (medullary and anaplastic cancers), are more difficult to quantify and therefore reliable staging methods are not available. The three most commonly used methods are described below.
It is important to note that the essence of all staging methods is that age is a major factor when determining prognosis. Young people rarely die of their disease regardless of whether the surrounding lymph nodes were affected, some of the tumor is not removed, the tumor extends into the veins or outside of the tissue which encapsulates it. However, for older patients all of these factors play a significant role in long term disease free survival.
Another important fact to keep in mind is that as long as the cancer is completely removed (remember that up to 70% of the time the cancer can be in both lobes of the thyroid gland), it makes no difference in survival if a portion of the thyroid or the entire thyroid is removed. Furthermore, for papillary cancer, many staging methods are not concerned with the spread (metastases) of cancer in the surrounding lymph nodes. This is because, thyroid cancer that spreads to the lymph nodes of the neck does not threaten survival at all. This is a difficult concept for many patients to understand, because for many other types of cancers, such as breast, colon and lung cancers, positive lymph nodes give you a worse prognosis, but is not true for papillary thyroid cancers.
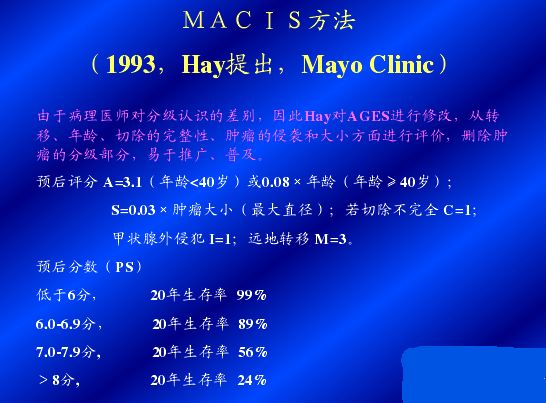
MAICS
The MAICS method was developed by the Mayo Clinic based on careful evaluation of a large group of patients. It is probably the most reliable staging method available and therefore most accurately predicts a patient\\\\"s outcome compared to other methods. It was developed to determine the prognosis of patients with papillary thyroid cancer. MAICS is an abbreviation for the factors taken into account to predict survival: (distant) Metastasis or spread of the cancer to areas outside the neck, Age of the patient at the time the tumor was discovered, Invasion of the cancerous tumor into surrounding areas of the neck as seen by the naked eye, (in)Completeness of surgical resection (or removal) of the tumor, and Size of the tumor. Each of these factors is mathematically scored as shown in the table below:
FACTORS
|
SCORE
|
distant Metastasis: Did the tumor spread to other parts of the body outside of the region of the neck?
|
yes = 3
no = 0 |
Age at the time the tumor was found
|
less than 39 years = 3.1
over 40 = 0.08 x age |
Invasion:Did the surgeon see that the tumor had extended beyond the thyroid into other regions of the neck?
|
yes = 1
no = 0 |
inComplete resection: Were there parts of the tumor that the surgeon was unable to remove (for example a part that was attached to the windpipe)?
|
yes = 1
no = 0 |
Size of tumor (measured by the pathologist)
|
0.3 x size in cm
|
Once the score for each factor is calculated, they are added up to get a total MAICS score and this total predicts the likelihood that the patient will live 20 years from the time the tumor was discovered. Fortunately most patients fall into the low risk category (MAICS score less than 6.0) and are cured of the cancer at the time of surgery.
20-year survival rate according to MAICS score
| ||||
MAICS Score
|
< 6.0
|
6.0 - 6.99
|
7.0 - 7.99
|
> 8.0
|
20 yr Survival
|
99%
|
89%
|
56%
|
24%
|
TNM
The TNM method is the most universally used staging method and applies to both papillary and follicular thyroid cancers. It was introduced in 1987 by the International Union Against Cancer and adopted by the American Joint Commission on Cancer. TNM stands for:
T: Tumor size (in cm). T=1 if the tumor is less than 1cm; T = 2 if it is 1-4 cm; T=3 if it is greater than 4 cm; and T=4 if the tumor extends beyond the thyroid gland.
N: Node metastasis - presence or absence of lymph node metastases (meaning has the cancer spread to the lymph nodes in the neck). If the cancer has spread to the lymph nodes, N = 1; if none of the lymph nodes were affected, N = 0
M: distant Metastases (meaning has the cancer spread beyond the neck to other areas of the body like the lung or bone) - if there is distant metastases, M = 1, if the cancer has not spread outside of the neck region, M = 0
Based on these three categories, the cancer is assigned a Stage of 1, 2 ,3 or 4. Stage 1 is the least advanced form of cancer with the best prognosis, and Stage 4 is the most advanced category. The table below shows the likelihood of a local recurrence (or recurrence of thyroid cancer in the neck region), distant recurrence (recurrence of cancer in other areas of the body), and mortality (death) based on the stage of a given tumor.
STAGE
|
AGE < 45
|
AGE > 45
|
Local Recurrence
|
Distant Recurrence
|
Mortality
|
I
|
Any T Any N M0
|
T1 N0 M0
|
5.5%
|
2.8%
|
1.8%
|
II
|
Any T Any N M1
|
T2 N0 M0
T3 N0 M0 |
7%
|
7%
|
11.6%
|
III
|
-
|
T4 N0 M0
Any T Any N M1 |
27%
|
13.5%
|
37.8%
|
IV
|
-
|
Any T Any N M1
|
10%
|
100%
|
90%
|
It is important to note that classifications made by a pathologist can be very subjective, particularly for tumors that have few distinctive characteristics, which is often the case with follicular cancer. For this reason, reliably staging a follicular thyroid cancer is more difficult because it is influenced by the subjective classification made by the pathologist. For example, some pathologists define a microscopic capsular invasion and a microscopic vascular invasion (minute extensions of the tumor which can only be seen under a microscope) as cancer while others may not.
AMES
Anther popular staging method is the AMES method, developed by the Lahey Clinic. Like the TNM method, it is applicable to both papillary and follicular thyroid cancers. This method takes into account the Age of the patient when the tumor was discovered, Metastases of the tumor to different sites other than neck lymph nodes, the Extent of primary tumor and, the Size of the tumor (if it is larger than 5 cm, or about 2 inches). Once these factors are determined, the patient is then placed into a high or low risk category, as shown in the table below:
LOW RISK
1.8% Mortality Rate |
HIGH RISK
46% Mortality Rate |
Men under 41 and Women under 51
without distant metastases |
All patients with distant metastases
|
All men over 41 and women over 51 with:
Intra-thyroidal papillary cancer (papillary cancer confined present only within the thyroid gland) ORfollicular cancer tumor with minor capsular involvement(the tumor slightly extends into the capsule which surrounds it) AND
Primary tumor less than 5 cm in diameter AND
No distant metastases
|
All men over 41 and women over 51 with:
Extra-thyroidal papillary cancer (extends beyond the thyroid gland) OR follicular cancer tumor with major capsular involvement(the tumor extends significantly into the capsule which surrounds it) AND/OR
Primary cancer is 5 cm in diameter or larger, regar
|
 点击放大图片
点击放大图片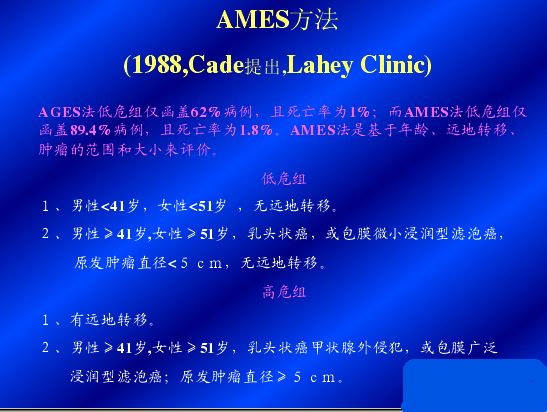 点击放大图片
点击放大图片 点击放大图片
点击放大图片
没有评论:
发表评论