From: "Handy, Susan" <Susan.Handy@fortbend.k12.tx.us>Subject: Congratulations again!!!Date: May 14, 2014 at 3:34:13 PM CDTTo: Rebecca Hu's mom <tiansma@yahoo.com>, Rebecca Hu's dad <huyuande@yahoo.com>Hi,Rebecca earned another Nitro the Chameleon sleepover!!! She was exceptionally polite and kind to her friends today and when there ended up being a 5 way tie she suggested that I let another student have it. She was so kind!Please congratulate her with me.Have a wonderful evening,Susan Handy2nd Grade TeacherCornerstone Elementary School1800 Chatham Ave.Sugar Land, Texas 77479281-634-6667
2014年5月21日星期三
2014年2月4日星期二
Tg undetected, no need further testing
Tg < 0.1 no need for testing
"This study is helpful because it indicates that for most patients with thyroglobulin values of <0.1 ng/ml while on thyroid hormone suppression, stimulated thyroglobulin testing is unnecessary since the likelihood of identifying residual cancer is very small. These findings will cut down on the need to perform stimulated thyroglobulin testing, which is both inconvenient for patients and expensive. Long term follow up of patients with thyroid cancer, however, still requires periodic measurement of thyroglobulin, since other studies indicate that ~4% of patients with initially undetectable basal thyroglobulin levels eventually had recurrent cancer."
http://www.thyroid.org/patient-thyroid-information/ct-for-patients/vol-7-is sue-2/vol-7-issue-2-p-7-8/
When thyroglobulin is undetectable, is any further testing needed in following patients with thyroid cancer?
"This study is helpful because it indicates that for most patients with thyroglobulin values of <0.1 ng/ml while on thyroid hormone suppression, stimulated thyroglobulin testing is unnecessary since the likelihood of identifying residual cancer is very small. These findings will cut down on the need to perform stimulated thyroglobulin testing, which is both inconvenient for patients and expensive. Long term follow up of patients with thyroid cancer, however, still requires periodic measurement of thyroglobulin, since other studies indicate that ~4% of patients with initially undetectable basal thyroglobulin levels eventually had recurrent cancer."
http://www.thyroid.org/patient-thyroid-information/ct-for-patients/vol-7-is sue-2/vol-7-issue-2-p-7-8/
When thyroglobulin is undetectable, is any further testing needed in following patients with thyroid cancer?
BACKGROUND
Thyroglobulin is a protein produced by both normal and cancerous thyroid cells. Treatment of thyroid cancer frequently involves total thyroidectomy and radioiodine therapy followed by thyroid hormone therapy to suppress serum TSH and turn off any residual normal thyroid cells. In this situation, the serum thyroglobulin level can be used as a thyroid cancer marker. Indeed, if any thyroid cancer cells are present, levels of thyroglobulin are often detectable, either on TSH suppression therapy or after stimulation with rhTSH (stimulated thyroglobulin testing). Measurement of thyroglobulin under these conditions has become standard practice in the follow up of patients with thyroid cancer. This study is an analysis of many other studies as to the usefulness of measuring serum thyroglobulin levels in managing patients with thyroid cancer.
Thyroglobulin is a protein produced by both normal and cancerous thyroid cells. Treatment of thyroid cancer frequently involves total thyroidectomy and radioiodine therapy followed by thyroid hormone therapy to suppress serum TSH and turn off any residual normal thyroid cells. In this situation, the serum thyroglobulin level can be used as a thyroid cancer marker. Indeed, if any thyroid cancer cells are present, levels of thyroglobulin are often detectable, either on TSH suppression therapy or after stimulation with rhTSH (stimulated thyroglobulin testing). Measurement of thyroglobulin under these conditions has become standard practice in the follow up of patients with thyroid cancer. This study is an analysis of many other studies as to the usefulness of measuring serum thyroglobulin levels in managing patients with thyroid cancer.
THE FULL ARTICLE TITLE: Giovanella L et al, Unstimulated high-sensitive thyroglobulin in follow-up of differentiated thyroid cancer patients: a meta-analysis. J Clin Endocrinol Metab. 2013 Nov 27.
SUMMARY OF THE STUDY
This study is an analysis of many other studies evaluating the utility of measuring thyroglobulin levels under thyroid hormone suppression therapy and after stimulation with rhTSH in patients with thyroid cancer. The authors identified 9 studies that used the newer, more sensitive thyroglobulin assay. These studies included a total of 3178 patients. The investigators found that when the basal thyroglobulin level under thyroid hormone suppression therapy is <0.1 ng/ml, it accurately predicts that the stimulated thyroglobulin level will be <1, which indicates absence of residual cancer cells.
This study is an analysis of many other studies evaluating the utility of measuring thyroglobulin levels under thyroid hormone suppression therapy and after stimulation with rhTSH in patients with thyroid cancer. The authors identified 9 studies that used the newer, more sensitive thyroglobulin assay. These studies included a total of 3178 patients. The investigators found that when the basal thyroglobulin level under thyroid hormone suppression therapy is <0.1 ng/ml, it accurately predicts that the stimulated thyroglobulin level will be <1, which indicates absence of residual cancer cells.
WHAT ARE THE IMPLICATIONS OF THIS STUDY? This study is helpful because it indicates that for most patients with thyroglobulin values of <0.1 ng/ml while on thyroid hormone suppression, stimulated thyroglobulin testing is unnecessary since the likelihood of identifying residual cancer is very small. These findings will cut down on the need to perform stimulated thyroglobulin testing, which is both inconvenient for patients and expensive. Long term follow up of patients with thyroid cancer, however, still requires periodic measurement of thyroglobulin, since other studies indicate that ~4% of patients with initially undetectable basal thyroglobulin levels eventually had recurrent cancer.
—M. Regina Castro, MD
ATA THYROID BROCHURE LINKS
Thyroid cancer: http://www.thyroid.org/cancer-of-the-thyroid-gland
Radioactive Iodine Therapy: http://www.thyroid.org/radioactive-iodine
2014年2月2日星期日
RAI on Small Differentiated Thyroid Cancer Having Microscopic Extrathyroidal Extension
Effects of Low-Dose and High-Dose Postoperative Radioiodine Therapy on the Clinical Outcome in Patients with Small Differentiated Thyroid Cancer Having Microscopic Extrathyroidal Extension
Background: It is unclear whether differentiated thyroid cancer (DTC) patients classified as intermediate risk based on the presence of microscopic extrathyroidal extension (ETE) should be treated with low or high doses of radioiodine (RAI) after surgery. We evaluated success rates and long-term clinical outcomes of patients with DTC of small tumor size, microscopic ETE, and no cervical lymph node (LN) metastasis treated either with a low (1.1 GBq) or high RAI dose (5.5 GBq).
Methods: This is a retrospective analysis of a historical cohort from 2000 to 2010 in a tertiary referral hospital. A total of 176 patients with small (≤2 cm) DTC, microscopic ETE, and no cervical LN metastasis were included. Ninety-six patients were treated with 1.1 GBq (LO group) and 80 patients with 5.5 GBq (HI group). Successful RAI therapy was defined as (i) negative stimulated thyroglobulin (Tg) in the absence of Tg antibodies, and (ii) absence of remnant thyroid tissue and of abnormal cervical LNs on ultrasonography. Clinical recurrence was defined as the reappearance of disease after ablation, which was confirmed by cytologically or pathologically proven malignant tissue or of distant metastatic lesions.
Results: There was no significant difference in the rate of successful RAI therapy between the LO and HI group (p=0.75). In a subgroup analysis based on tumor size, success rates were not different between the LO group (34/35, 97%) and the HI group (50/56, 89%) in patients with a tumor size of 1–2 cm (p=0.24). In patients with smaller tumor size (≤1 cm), there was no significant difference in success rates between the LO (59/61, 97%) and HI group (22/24, 92%; p=0.30). No patient had clinical recurrences in either group during the median 7.2 years of follow-up.
Conclusions: Low-dose RAI therapy is sufficient to treat DTC patients classified as intermediate risk just by the presence of microscopic ETE.
===============
Users who read this article also read
 |
|
|
|
|
|
甲状腺癌风险分级评分系统
Stage III papillary thyroid cancer
Stage III is papillary carcinoma in patients older than 45 years that is larger than 4 cm and is limited to the thyroid or with minimal extrathyroid extension, or positive lymph nodes limited to the pretracheal, paratracheal, or prelaryngeal/Delphian nodes. Papillary carcinoma that has invaded adjacent cervical tissue has a worse prognosis than tumors confined to the thyroid.
----------------Pathology report
tumor #1 with focal extension into soft tissue immediately surrounding thyroid.
发表者:龙斌 3179人已访问
any staging methods have been developed in order to predict the prognosis for a patient with differentiated thyroid cancer. These methods quantify various characteristics of the individual tumor as well as the patient. Fortunately most types of thyroid cancer have an excellent prognosis. Unlike other types of cancer, the prognosis of differentiated thyroid cancer largely depends on the age of the patient at the time it is diagnosed. Thyroid cancers which are not differentiated (medullary and anaplastic cancers), are more difficult to quantify and therefore reliable staging methods are not available. The three most commonly used methods are described below.
It is important to note that the essence of all staging methods is that age is a major factor when determining prognosis. Young people rarely die of their disease regardless of whether the surrounding lymph nodes were affected, some of the tumor is not removed, the tumor extends into the veins or outside of the tissue which encapsulates it. However, for older patients all of these factors play a significant role in long term disease free survival.
Another important fact to keep in mind is that as long as the cancer is completely removed (remember that up to 70% of the time the cancer can be in both lobes of the thyroid gland), it makes no difference in survival if a portion of the thyroid or the entire thyroid is removed. Furthermore, for papillary cancer, many staging methods are not concerned with the spread (metastases) of cancer in the surrounding lymph nodes. This is because, thyroid cancer that spreads to the lymph nodes of the neck does not threaten survival at all. This is a difficult concept for many patients to understand, because for many other types of cancers, such as breast, colon and lung cancers, positive lymph nodes give you a worse prognosis, but is not true for papillary thyroid cancers.
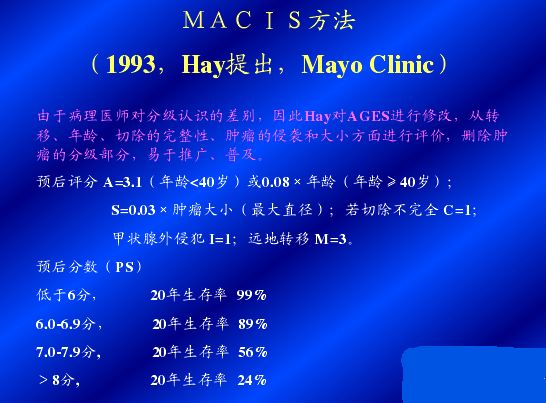
MAICS
The MAICS method was developed by the Mayo Clinic based on careful evaluation of a large group of patients. It is probably the most reliable staging method available and therefore most accurately predicts a patient\\\\"s outcome compared to other methods. It was developed to determine the prognosis of patients with papillary thyroid cancer. MAICS is an abbreviation for the factors taken into account to predict survival: (distant) Metastasis or spread of the cancer to areas outside the neck, Age of the patient at the time the tumor was discovered, Invasion of the cancerous tumor into surrounding areas of the neck as seen by the naked eye, (in)Completeness of surgical resection (or removal) of the tumor, and Size of the tumor. Each of these factors is mathematically scored as shown in the table below:
FACTORS
|
SCORE
|
distant Metastasis: Did the tumor spread to other parts of the body outside of the region of the neck?
|
yes = 3
no = 0 |
Age at the time the tumor was found
|
less than 39 years = 3.1
over 40 = 0.08 x age |
Invasion:Did the surgeon see that the tumor had extended beyond the thyroid into other regions of the neck?
|
yes = 1
no = 0 |
inComplete resection: Were there parts of the tumor that the surgeon was unable to remove (for example a part that was attached to the windpipe)?
|
yes = 1
no = 0 |
Size of tumor (measured by the pathologist)
|
0.3 x size in cm
|
Once the score for each factor is calculated, they are added up to get a total MAICS score and this total predicts the likelihood that the patient will live 20 years from the time the tumor was discovered. Fortunately most patients fall into the low risk category (MAICS score less than 6.0) and are cured of the cancer at the time of surgery.
20-year survival rate according to MAICS score
| ||||
MAICS Score
|
< 6.0
|
6.0 - 6.99
|
7.0 - 7.99
|
> 8.0
|
20 yr Survival
|
99%
|
89%
|
56%
|
24%
|
TNM
The TNM method is the most universally used staging method and applies to both papillary and follicular thyroid cancers. It was introduced in 1987 by the International Union Against Cancer and adopted by the American Joint Commission on Cancer. TNM stands for:
T: Tumor size (in cm). T=1 if the tumor is less than 1cm; T = 2 if it is 1-4 cm; T=3 if it is greater than 4 cm; and T=4 if the tumor extends beyond the thyroid gland.
N: Node metastasis - presence or absence of lymph node metastases (meaning has the cancer spread to the lymph nodes in the neck). If the cancer has spread to the lymph nodes, N = 1; if none of the lymph nodes were affected, N = 0
M: distant Metastases (meaning has the cancer spread beyond the neck to other areas of the body like the lung or bone) - if there is distant metastases, M = 1, if the cancer has not spread outside of the neck region, M = 0
Based on these three categories, the cancer is assigned a Stage of 1, 2 ,3 or 4. Stage 1 is the least advanced form of cancer with the best prognosis, and Stage 4 is the most advanced category. The table below shows the likelihood of a local recurrence (or recurrence of thyroid cancer in the neck region), distant recurrence (recurrence of cancer in other areas of the body), and mortality (death) based on the stage of a given tumor.
STAGE
|
AGE < 45
|
AGE > 45
|
Local Recurrence
|
Distant Recurrence
|
Mortality
|
I
|
Any T Any N M0
|
T1 N0 M0
|
5.5%
|
2.8%
|
1.8%
|
II
|
Any T Any N M1
|
T2 N0 M0
T3 N0 M0 |
7%
|
7%
|
11.6%
|
III
|
-
|
T4 N0 M0
Any T Any N M1 |
27%
|
13.5%
|
37.8%
|
IV
|
-
|
Any T Any N M1
|
10%
|
100%
|
90%
|
It is important to note that classifications made by a pathologist can be very subjective, particularly for tumors that have few distinctive characteristics, which is often the case with follicular cancer. For this reason, reliably staging a follicular thyroid cancer is more difficult because it is influenced by the subjective classification made by the pathologist. For example, some pathologists define a microscopic capsular invasion and a microscopic vascular invasion (minute extensions of the tumor which can only be seen under a microscope) as cancer while others may not.
AMES
Anther popular staging method is the AMES method, developed by the Lahey Clinic. Like the TNM method, it is applicable to both papillary and follicular thyroid cancers. This method takes into account the Age of the patient when the tumor was discovered, Metastases of the tumor to different sites other than neck lymph nodes, the Extent of primary tumor and, the Size of the tumor (if it is larger than 5 cm, or about 2 inches). Once these factors are determined, the patient is then placed into a high or low risk category, as shown in the table below:
LOW RISK
1.8% Mortality Rate |
HIGH RISK
46% Mortality Rate |
Men under 41 and Women under 51
without distant metastases |
All patients with distant metastases
|
All men over 41 and women over 51 with:
Intra-thyroidal papillary cancer (papillary cancer confined present only within the thyroid gland) ORfollicular cancer tumor with minor capsular involvement(the tumor slightly extends into the capsule which surrounds it) AND
Primary tumor less than 5 cm in diameter AND
No distant metastases
|
All men over 41 and women over 51 with:
Extra-thyroidal papillary cancer (extends beyond the thyroid gland) OR follicular cancer tumor with major capsular involvement(the tumor extends significantly into the capsule which surrounds it) AND/OR
Primary cancer is 5 cm in diameter or larger, regar
|
 点击放大图片
点击放大图片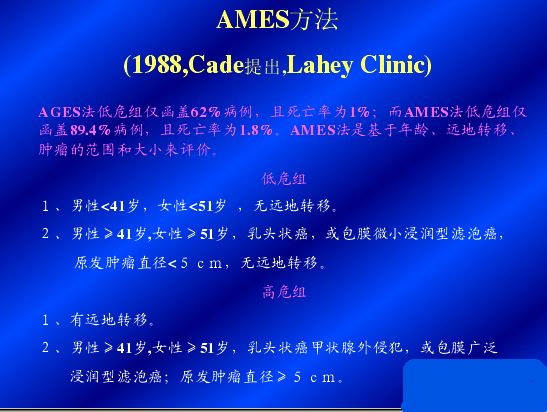 点击放大图片
点击放大图片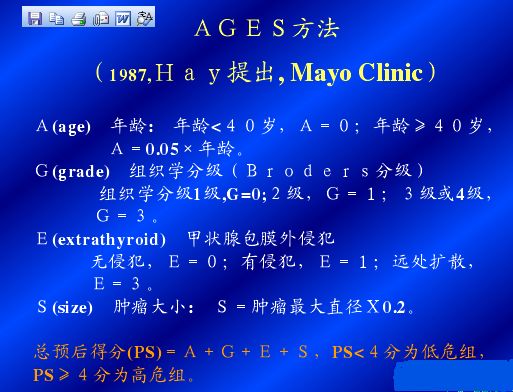 点击放大图片
点击放大图片RAI for node negative PTC with capsular invasion only
Here's a new study which found that RAI treatment doesn't affect the recurrence rate for patients with microscopic capsular invasion:
http://onlinelibrary.wiley.com/doi/10.1111/ajco.12159/abstract;jsessionid=C 8E8BD1F53EC125912D7470200CA70B0.f03t04?deniedAccessCustomisedMessage=&userI sAuthenticated=false
http://onlinelibrary.wiley.com/doi/10.1111/ajco.12159/abstract;jsessionid=C 8E8BD1F53EC125912D7470200CA70B0.f03t04?deniedAccessCustomisedMessage=&userI sAuthenticated=false
Abstract
Aim
With thyroid carcinoma the decision to use radioactive iodine (RAI) ablation depends on the risk of poor outcomes. Although extrathyroid extension (ETE) is well known as a risk of poor outcomes for papillary thyroid carcinoma (PTC), the definition of minimal ETE is too broad, as it encompasses both microscopic invasion of the thyroid capsule (capsular invasion [CI]) and macroscopic invasion of the sternothyroid muscle.
Methods
We conducted a retrospective study to analyze the prognostic benefit of RAI ablation according to the presence of CI in a consecutive series of patients with PTC between October 1997 and December 2008. We studied two groups of patients, including those who received RAI (group I, n = 121) and those who did not (group II, n = 108). During follow-up, we assessed the locoregional recurrence of all patients.
Results
There were no statistically significant difference between the groups regarding locoregional recurrence at follow-up (13.2% for group I vs 9.3% for group II, P = 0.441). The association between RAI and locoregional recurrence in PTC patients with CI remained insignificant after adjusting for potential confounders, such as age, tumor size, sex, lymphatic invasion, vascular invasion and tumor multiplicity (P = 0.409, hazard ratio = 0.698, 95% confidence interval, 0.298–1.639).
Conclusions
This retrospective study suggests that RAI treatment is not associated with less locoregional recurrence in PTC patients who only demonstrate CI, although further prospective studies are required to confirm these findings.
2014年1月25日星期六
Reduction of Cholesterol by Alternative Therapies
Abstract
Although synthetic chemicals and pharmacological agents are being used for the treatment of cardiovascular disease in the western world, there now appears to be a cultural and philosophical shift toward Eastern Medicine and many patients are increasingly using alternative approaches for prevention and therapeutic purposes. This brief review summarizes the experimental and clinical evidence of some functional foods, herbal products and medicinal plants for improving plasma HDL cholesterol, LDL cholesterol, triglycerides and glucose levels, as well as reducing oxidative stress. In addition, the potential of acupuncture and Yogic meditation are discussed as emerging approaches for reducing cardiovascular disease risk factors. The available evidence indicates that several functional foods, herbal products and medicinal plants exert lipid-lowering and hypoglycemic actions, as well as exhibit antioxidant properties; however, a great deal of research work and extensive clinical trials are needed to establish their use in medical practice.
Introduction
The accumulation of lipids within arteries remains the initial stimulus for the pathogenesis of atherosclerosis; however, oxidative stress is also considered to play a critical role in this process.[1]Several lipid-lowering drugs, such as statins, are used as the first-line therapy in hypercholesterolemia.[2]Statin monotherapy is generally well tolerated; however, a low frequency occurrence of myopathy and asymptomatic increase in hepatic transaminases have been reported.[2] In addition, since statins are prescribed on a long-term basis, drug–drug interactions are possible, since many of the patients that receive statins may also be prescribed other medications for concomitant conditions.[2] In a study on cholesterol-lowering statin drugs (all types) involving 150,000 postmenopausal women, aged 50–79, it was found that statin intake was linked to a 48% increase in the risk of developing diabetes.[3]Furthermore, statin use was linked to an even higher risk of diabetes in Hispanic and Asian women, at 57 and 78% higher, respectively, and women who were not overweight (and thus not at risk of developing diabetes) were at a similar risk as women who were overweight for developing diabetes. Interestingly, it has been suggested that while statins are of benefit for people with known heart disease, they may be of no benefit to individuals without known heart disease and are attempting to control their blood cholesterol levels.[4]
On the other hand, the use of herbal and medicinal plant products has gained popularity as preventive or therapeutic agents for cardiovascular disease (CVD). Herbs are generally defined as any form of plant or plant products that are regarded as food or natural health products. Herbal supplements have been used for medicinal purposes for thousands of years in the East, particularly the Ayurvedic system and the Chinese medicine, and have recently become popular among consumers in the west.[5] It should be mentioned that Ayurveda is derived from two Sanskrit words, namely 'Ayus' and 'Veda,' meaning life and knowledge, respectively. It is a holistic system that focuses on the body, mind and conscious. Ayurvedic treatment consists of the use of herbal preparations and emphasizes the practice of yoga and meditation.[6] The traditional Chinese medicine is based on 'Zheng' system for the control of overall function of the human body and emphasizes the use of acupuncture and that practice of qigong.[7] Herbal medicines including traditional Chinese and Ayurvedic medicines are considered to be cost-effective in the management of disease and this alternative form of medical practice differs in philosophy from the modern medicine, and is known to play an important role in health maintenance.[8]
In the holistic approach to health care, both the disease and the underlying causes are being controlled through physical, mental, social and spiritual well-being. Although these alternative therapies are gaining popularity, several issues regarding safety and efficacy of herbal medicines remain to be addressed.[5,9,10] Since elevated levels of plasma total cholesterol, LDL cholesterol (LDL-C), triglycerides (TGs) and glucose are well-known risk factors for coronary artery disease (CAD), this brief review is focused on some of the alternative therapies for improving blood lipid profile and glucose levels. While it has been argued that it is not only native LDL that contributes to atherosclerosis, but the amount of oxidized LDL that is a key contributor to atherosclerosis,[1] this article will therefore also discuss the possible antioxidants effects of functional foods, herbal products and medicinal plants. In view of the role of diabetes as a major risk factor for CVD, this article will also discuss the hypoglycemic and hypolipidemic effects of these therapies during diabetes.
The selected therapies are based on the availability of clinical evidence on efficacy, with respect to improvements in the plasma profiles of total cholesterol, HDL cholesterol (HDL-C), LDL-C (native and oxidized forms) and TGs, as well as glucose-lowering and antioxidant effects (Figure 1). These natural products deserve further work to isolate and characterize their constituents for the development of novel and more effective agents. A consideration for acupuncture, as well as yoga, is also presented as emerging alternative approaches in preventing/treating CVD.

2014年1月20日星期一
Synthroid vs. Tirosint
http://bbs.wenxuecity.com/thyroid/263514.html
我在41岁时,有过一次甲状腺发炎,吞咽困难,发烧,几天后逾越,做过同位素检查,无异样病变,但是从这以后,便开始了我十几年与甲状腺低下抗争的漫漫的路程。
甲状腺低下是一种内分泌失调疾病,症状是新陈代谢降低,精神不振,怕冷,反应迟钝,体重增加,检测指标是TSH(甲状腺刺激荷尔蒙)高于4.5。 这种疾病很常见,在生育以后的妇女中高达13%,治疗方案是吃Synthroid, 补充甲状腺,要终身吃药。开始几年,我可以吃Synthroid,没有什么反应,医生将剂量调到合适,控制TSH在正常值内。
到我过了50岁后,开始有了睡眠问题,Synthroid吃下后太兴奋,难以入睡,我便停了药,睡眠好转,但是TSH指标上升,不能不理会。医生认为Synthroid不会造成睡眠障碍,开一些安眠药给我吃,吃安眠药会成瘾,自己心里有阴影。 这种情况持续了好几年,我的TSH高到了17,家庭医生很不同意我停药,虽然我的症状还不明显。我也到国内看过内分泌专科医生,结论一样,不能停药,睡眠问题另外解决,可以用些五味子等中药,但是效果较慢,不能解决根本问题。那段时间其实我的状况不好,睡眠和甲状腺指标均不好。
到了2009春,工作压力很大,回国一次,家中照顾老母亲的保姆老是搞不定,加上中美来回两边倒时差,睡眠很差,体重持续下降,思想无法集中,我意识到自己出现了忧郁症症状,并且伴有手发抖的现象,我觉得不能再服用Synthroid了,验血后,TSH指标在6左右,虽然还是高了些,但是我的身体长期在甲状腺低下的状态,已经不适应接近正常的水平了,这时我的专科医师同意我停了Synthroid,观察一段时间。另外她提议我验维他命D,若是维他命很低的话,是会造成浑身无力的感觉,可以吃大剂量处方维他命D。验出来的D非常低,医生给我开了药。后来,我请教了在制药公司工作的朋友,她告诉我,最新研究发现,甲状腺问题加上维他命D低下,有可能激发忧郁症。我与此位朋友相知多年,她说我不像会得忧郁症的人,这条消息给了我一些帮助,当时自己一直在“我怎么会变成这样?”的怪圈中走不出来,关于这一段心路历程,我纪录在了“失而复得—从忧郁症中走出来”一文中。
自知甲状腺终究是个问题,等我走出了忧郁症,睡眠也变好后,我开始吃一些Synthroid,反应大,总吃不到医生要求的剂量。 2010年中开始,体重直线上升,四个月中增了15磅,中老年妇女的这段时期是比较难过的,我也搞不清是甲状腺问题还是更年期发胖,验血后吓一跳,TSH高到55,赶紧去看专科医师,她给我换了一个药,叫作 Tirosint,50毫微克,她认为还是不够,但是让我先服用,两个月后再去看。我吃了没有反应,睡眠正常,也没有过于饥饿的感觉,心里障碍解除了,我认认真真吃了两个月,心里非常感谢这位专科医师。我在与忧郁症抗争时,体会到药是否对路太重要了,也感到找一位高明的医师的必要,所以这一次也是认真对待。两个月后,TSH降至9,医师继续加剂量,到达75毫微克,但是让我看身体反应,不适应的话,可以回到50毫微克。我自己调整一下,大概是三天吃75毫微克,一天吃50毫微克,人感到轻松些了,于是加强锻炼,节制饮食,体重开始慢慢下降,自我感觉良好。
又过了6周,我的TSH降到3.0,正常范围是0.45 – 4.5。 这是十几年以来第一次降到正常值,我向医师表示由衷的钦佩和感谢,医师也很高兴,她说两个药的主要成分是一样的,填料不同。但是就是这个填料不被我的身体接受,才让我受了那么多年的痛苦。医师说我可以保持我的交换服药法,只需四个月以后去看她,她还说,TSH降到1--2,人会感到轻松有活力。
告别医师,我心情愉快地回家,几年磨练,总算修得正果,以后不用老是去看医生,真是一件好事。人的新陈代谢机能恢复后,会影响到各方面,譬如,我不再那么怕冷,不是那么老是觉得口渴,头发脱落减少了,体重略下降,人感到轻松了,还有的指标照理与甲状腺无关,但是我的血压,胆固醇,血脂都变好了,其中胆固醇十几年来第一次降到200以下。现在下了班,我还可以做饭,晚饭后整理花园,然后走半小时。我看待事物也正面积极了,虽然生活中总有不顺利的事,但是有了健康,不就是最大的幸事么?这次的甲状腺指标恢复正常,还真让我兴奋了好几天。
在经过了这漫长的过程,有几点体会,
- 第一是我们要尊重科学,指标不好也许还没有反应到身体其它部分,但是长期下去是不行的,后果严重。甲状腺低下在中国国内的重视还不如西方国家,忠告有同样疾病的同胞,一定要积极对待;
- 第二,美国的医生水平还是不错,敬业而且尊重病患的感觉,即使我讲得不对,他们也不会训斥讥笑你,很是和蔼可亲。像Synthroid这个药,是一个很成熟的药,对绝大部分患者都适用,若是在国内,医生不会听得进我的抱怨,但是我的医生配合我的需要换了新药。在美国医学院,专门教授“医患关系”课程,医生提供服务,病人是他们的市场,这比在国内看病受气要好很多;
- 第三,自己要配合,要钻研,我有一次的TSH指标非常高,后来我听了电台中的医学讲座,发现吃Synthroid时,四小时之内不能服钙片,我改正后,指标马上低了下来,后来又发现,其实这一点标在药瓶上,因为字体小,是我忽略了。我也在网上看病友的文章,发现也有人与我一样,不能吃Synthroid,病友们鼓励你将感觉和建议和医生交流,有人甚至因为医生听不进建议,将医生炒了鱿鱼,另外找了一个。
在此将自己的经历写出来,希望能惠益他人,不必花那么大的代价,走那么曲折的路,才找到合适的治疗方案。
======================
青竹叶2011-04-15 06:31:22回复悄悄话回复nightrose的评论:
说得好,当时我的家庭医生没有让我转去看专科医生,耽误了。 至于我目前服用的Tirosint,好像是新近才批准上市的,2009年时专科医师提起过“Armor”。这一类药的选择并不多
nightrose2011-04-13 10:06:06回复悄悄话楼主刚得病时就应该多查查医学资料,看看各路专家对用药的建议。我也得过急性甲状腺发炎,最初医生也没有确诊,在瞎猜我是不是扁桃体发炎等等。我在网上查过资料后去建议医生作化验,才诊断出来。治疗过程中我也不断查资料,确保知道自己的病是怎么一回事。
网上有各种甲状腺激素口服药的明确比较。一种药不行应该试另一种,怎么能等好几年?
======================
青竹叶2011-04-15 06:31:22回复悄悄话回复nightrose的评论:
说得好,当时我的家庭医生没有让我转去看专科医生,耽误了。 至于我目前服用的Tirosint,好像是新近才批准上市的,2009年时专科医师提起过“Armor”。这一类药的选择并不多
nightrose2011-04-13 10:06:06回复悄悄话楼主刚得病时就应该多查查医学资料,看看各路专家对用药的建议。我也得过急性甲状腺发炎,最初医生也没有确诊,在瞎猜我是不是扁桃体发炎等等。我在网上查过资料后去建议医生作化验,才诊断出来。治疗过程中我也不断查资料,确保知道自己的病是怎么一回事。
网上有各种甲状腺激素口服药的明确比较。一种药不行应该试另一种,怎么能等好几年?
2014年1月5日星期日
订阅:
博文 (Atom)